What does it take for a Hispanic RA patient to actually trust health education?
Not just receive it, but engage with it, complete it, and carry it into the exam room. This case study documents what Hispanic Healthbridge learned across a two-year, $1 million national program: the answer involves the physician, the phone, the language, the format, and the visit that comes after.
The IRB-approved methodology behind this program is the evidence FDA reviewers want to see in a DAP.
A diversity action plan that references peer-reviewed methodology, IRB-approved program design, and published retention outcomes carries a credibility signal that generic health equity consulting cannot provide. The HOPE-CAPE program is that evidence base: published in RMD Open, presented at ACR Convergence, and built around the mobile-first, Spanish-first design principles that characterize a defensible Phase 3 patient education component. When FDA reviewers evaluate whether a recruitment program will actually reach Hispanic patients, this is the kind of documented methodology they are looking for.
FDA Diversity Action Plan Advisory →Patient education that is prescribed gets completed
The program was designed around a clinical insight: patient education that is not prescribed by the physician does not get completed. The solution was to make the educational module part of the clinical encounter itself.
Rheumatologists participating in the program formally "prescribed" the educational module to their Hispanic RA patients, integrating it into the visit workflow rather than leaving it as optional follow-up. At the same visit, both the physician and the patient completed an independent baseline assessment.
The physician completed a Physician Patient-Reported Outcome (PPRO) survey evaluating their perception of the visit and the patient's engagement. Simultaneously, the patient completed a Patient-Reported Outcome (PRO) survey on a separate tablet, assessing the same visit from their own perspective. Neither saw the other's responses.
How the workflow ran
At the clinical visit, rheumatologist prescribes the module. Both physician and patient complete independent baseline surveys (PPRO and PRO) without seeing each other's responses. Between visits, patient completes modules on their phone. At the follow-up visit, both complete the same surveys again. Results compared.
How patients received the program
After the clinical visit, patients received the educational modules through the channel they already used: their phone. Module delivery was multimodal and in conversational, idiomatic Spanish, not translated English.
Content was delivered across WhatsApp messages, short-form video, and social-format educational cards, matching the finding that Hispanic RA patients prefer video, podcast, graphic, and article formats over text-only materials. Patients were nudged by phone to complete the modules between visits, designed to feel like a trusted contact following up, not an automated reminder.
"We found that even when patients identified trustworthy information in Spanish, it was more effective overall to present the same material in various ways such as articles, videos, podcasts, graphics, and more. In addition, our program materials were written using conversational, idiomatic Spanish, which patients found more useful and trustworthy than materials simply translated from their original English."
— Daniel Hernandez, MD, lead study author, GHLF Q4 2022 Quarterly Report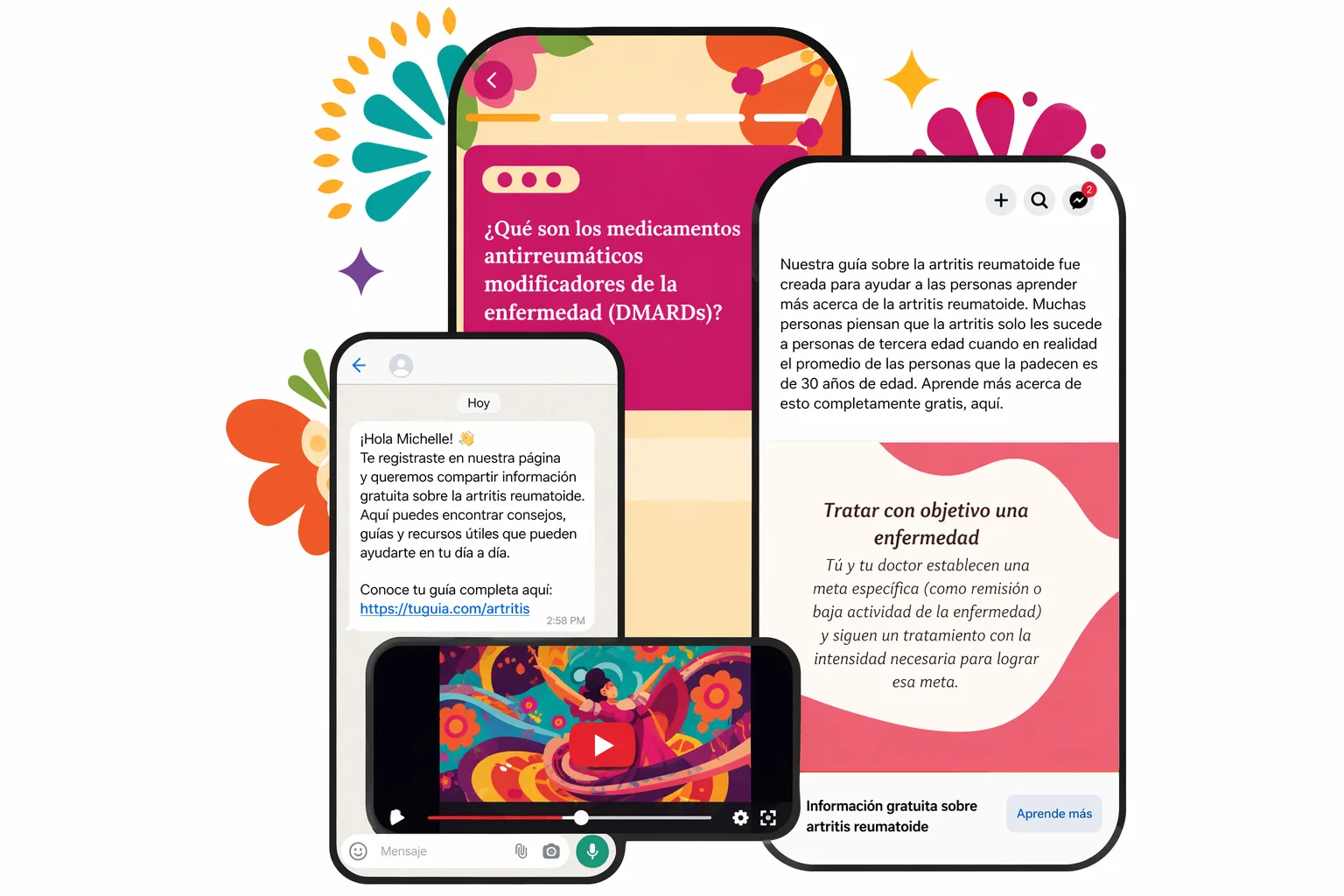
The multimodal delivery approach: WhatsApp nudges, Spanish-language video education, and social-format RA content cards, all designed for completion on a phone.
The educational module patients completed
This is the same interactive assessment tool embedded in the HOPE-CAPE RA program, bilingual, mobile-friendly, and built around real RA patient education content. Both English and Spanish versions are available.
What the next visit showed
At the follow-up clinical visit — after patients had completed the modules, both the physician and the patient completed the same PPRO and PRO surveys again.
The results showed that on the visit following module completion, both the physician and the patient independently reported more positive perception scores compared to the baseline visit. The physician perceived the patient as more engaged and better prepared. The patient reported feeling more informed and more confident in the clinical conversation.
This is the core proof of value: a mobile-first, multimodal, Spanish-first educational program did not just reach patients. It changed the quality of the clinical encounter that followed.
The finding
On the visit following module completion, both the physician (PPRO) and the patient (PRO) independently reported improved perception scores versus baseline. Neither saw the other's survey responses. The improvement was mutual and independently documented.
Publications and presentations
This program produced peer-reviewed publications, ACR Convergence presentations, and a follow-on study built from over 1,000 patients.
- ACR Convergence 2022: Oral Presentation "Exploring Patient Journeys and Education Needs of Hispanic Individuals with Rheumatoid Arthritis," Arthritis & Rheumatology 2022; 74 (suppl 9). First-authored abstract; covered by HCPLive following presentation.
- ACR Convergence 2022: Poster (Almonacid et al.) Patient advisory board retention documented as 100% across the full two-year program. PAB structure and engagement protocol described.
- ACR Convergence 2023: Co-Led Study "Feasibility and Efficacy of Culturally Appropriate Spanish Language-First Patient Education for Rheumatoid Arthritis." Built from feedback from more than 1,000 Hispanic patients who completed the initial program.
- RMD Open (2021): Peer-Reviewed Publication Co-authored with Hyon K. Choi, Jasvinder A. Singh, and Robert Terkeltaub. DOI: 10.1136/rmdopen-2021-001623.
The prescription model changes the clinical encounter
The case for physician-integrated patient education
The program proved that when a physician prescribes education, when that education arrives in the patient's language and preferred format, and when it is completed before the next visit, both sides of the clinical relationship improve. That is not a communication insight. It is a clinical outcomes insight.
For pharma medical affairs teams, research organizations, and patient advocacy foundations, this program is a demonstration of what separates patient education that changes behavior from patient education that merely exists. The difference is not budget or production value. It is whether the program was designed around how Hispanic patients actually receive and trust information.
What this model delivers
- Physician-integrated workflow that makes completion structurally likely, not optionally hopeful.
- Multimodal, Spanish-first content that patients find more useful than translated material.
- Dual-sided PRO/PPRO measurement that captures the impact on both patient and physician.
- IRB-approved methodology producing publishable, conference-ready research outputs.
- 100% patient advisory board retention, a design standard, not a happy accident.
Build Hispanic outreach that actually performs
Whether you are designing a disease-specific campaign, closing enrollment gaps, or building a foundation for long-term Hispanic patient engagement, Dr. Hernandez can help you get it right from the start.